Headaches are often triggered and/or aggravated by a constellation of muscles of the neck that contain taut bands, trigger points and other dysfunctional segments. Understanding the relationships between these muscles helps determine approaches for treatment and as well as self-care.
The muscles of the neck are part of a myofascial system that includes not only an anatomical but also a functional continuum. This means that a dysfunction of one muscular portion will result in a functional alteration of all the muscles of the neck. This must be taken into account for a successful resolution of the problem.
Major Muscle Groups
There are three groups of muscles that cause much of this pain directly. In addition, these muscles tend to cause satellite trigger points and dysfunctional patterns in other muscles of the head, neck, shoulder and arm.
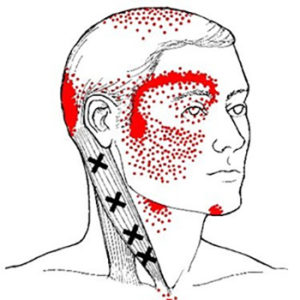 The two different branches of the SCM, the "sternal" (pictured above) and the "clavicular" provide direct referral patterns that cover large areas of the face and head.
The two different branches of the SCM, the "sternal" (pictured above) and the "clavicular" provide direct referral patterns that cover large areas of the face and head.
 Dysfunction in the SCM can cause headaches, facial pain and autonomic responses such as changes to the function or perception of the eyes and ears. This includes tearing, fluttering of the eyelids, unilateral deafness, tinnitus and vertigo.
Even worse, the SCM tends to induce satellite disturbances in other muscles within its referral zone. An unhappy SCM can cause a cascade of problems.
Dysfunction in the SCM can cause headaches, facial pain and autonomic responses such as changes to the function or perception of the eyes and ears. This includes tearing, fluttering of the eyelids, unilateral deafness, tinnitus and vertigo.
Even worse, the SCM tends to induce satellite disturbances in other muscles within its referral zone. An unhappy SCM can cause a cascade of problems.
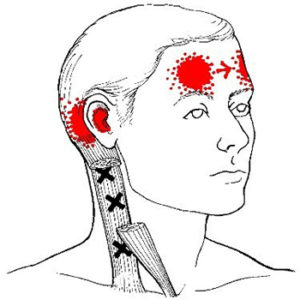
 Pain patterns of the upper trap include the temples and the side/back of the neck. The similarities to aspects of the SCM pattern are no accident. In embryological development, the trapezius and sternocleidomastoid muscle form separately from most other muscles as a singular mass. The two muscles split around the 20th week but retain common nerve connections.
Pain patterns of the upper trap include the temples and the side/back of the neck. The similarities to aspects of the SCM pattern are no accident. In embryological development, the trapezius and sternocleidomastoid muscle form separately from most other muscles as a singular mass. The two muscles split around the 20th week but retain common nerve connections.
The trapezius is actually divided into upper, middle and lower sections and taut bands and trigger points in the lower sections can refer to the neck and interfere with treating the upper trap. The trapezius can, in turn, induce satellite trigger points and dysfunctional areas in muscles such the SCM and posterior neck group.
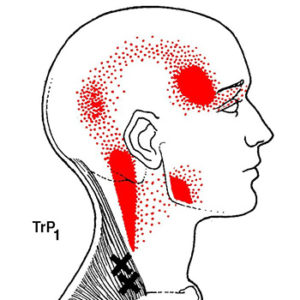
 Distribution of pain patterns include the top/back of the head, the temples and back of the neck. In fact, if you overlay the pain patterns of the posterior neck muscles with the SCM and trapezius there are quite a lot of areas in common.
Distribution of pain patterns include the top/back of the head, the temples and back of the neck. In fact, if you overlay the pain patterns of the posterior neck muscles with the SCM and trapezius there are quite a lot of areas in common.
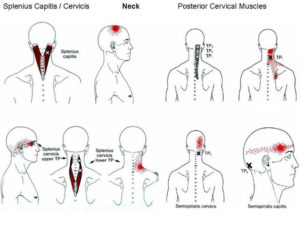
The cervical spinal erectors, semispinalis cervicis and capitis, work in concert with splenius cervicis and capitis group and others, to provide postural support, rotation, side flexion and extension of the neck. Other muscles in the referral zone of these muscles include the SCM and trapezius, so it is easy to see how the can all participate in a cycle of dysfunction.
Associated Trigger Points and Dysfunction
 Major satellites of the SCM include the masseter and temporalis (used in chewing), the trapezius and posterior cervical muscles and smaller muscles of the front of the neck, such as the scalenes (respiratory muscles) and the infrahyoids and suprahyoids (used in swallowing and speech). Some of these, in turn can cause issues in the shoulder and arm.
Major satellites of the SCM include the masseter and temporalis (used in chewing), the trapezius and posterior cervical muscles and smaller muscles of the front of the neck, such as the scalenes (respiratory muscles) and the infrahyoids and suprahyoids (used in swallowing and speech). Some of these, in turn can cause issues in the shoulder and arm.
Common satellites of the trapezius include different segments within itself, such as the lower trap inducing dysfunction in the upper trap, levator scapulae and muscles of the shoulder. The larger posterior neck muscles may cause tight bands and trigger points to develop in the small cervical multifidi and sub-occipital muscles,
An individual has headaches behind the eyes and at the temples on both sides and pain in the back of the neck on the right side. They can rotate the head/neck pretty well and there is no popping or pain with opening the jaw or chewing. During postural evaluation we have noted consistent forward flexion of the neck. It also came up that there is an A/C vent pretty much directly over the individual at work.
We start considering the SCM, lower and upper trapezius, semispinalis capitis and upper portion of splenius cervicis on both sides to address the pain at the temples. For the neck pain on the right, we would treat the 2nd (lower) trigger points of splenius cervicis and the upper trap and in the multifidi of the neck on the right side. I would probably treat these muscles in approximately reverse order, ending with the SCM.
The goal is to release trigger points and taut bands so that muscles that are locked short can lengthen, and those that are locked long can shorten and regain their normal tone. We would typically perform trigger point compression and myofascial release and movement through the entire range of motion of these muscles.
Self care would focus on gentle stretching and disengagement of the SCM and strengthening of the lower traps and deep cervical flexors in the front of the neck. This will allow the upper traps and posterior cervical muscles to return to normal length and tone. Finally, we’re suggesting moving the desk or diverting the vent that is blowing on the back of the neck; this is known to cause trouble with some neck muscles.
Neck issues can be complicated, with a significant number of muscles involved. Focus on key elements that directly impact the primary issues you are facing. Self-compression is the foundation of myofascial self-care. However, in dealing with the neck, it is important to respect the delicacy of the area. Be gentle with yourself!
Do not use ice on your neck! For most other areas of the body, ice can be used safely and effectively to reduce inflammation. However, because cold can activate known trigger points in certain neck muscles, we avoid ice in this area.
Limit stretches to the appropriate areas. Not every “tight” muscle benefits from stretching. For instance, prolonged flexion of the neck makes posterior neck muscles feel tight from being over-stretched. Further stretching will not help. These muscles are “locked long” and need to be reset to their normal length through compression, muscle activation and restoring range of motion on the shorter end. Gentle stretching of the front of the neck, including the SCM, will be more effective than stretching the back of the neck, no matter how “tight” it might be.
If you are having similar issues, you may find that a session or two to identify and treat root causes of your individual case is helpful. Call us at 630-858-0000 today to make an appointment!
Extra – Neck Muscle Anatomy
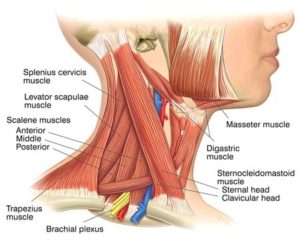
 The sternocleidomastoid muscle is one of the largest and most superficial cervical muscles. The primary actions of the muscle are rotation of the head to the opposite side and flexion of the neck. The sternocleidomastoid is innervated by the accessory nerve.
It is given the name sternocleidomastoid because it originates from the top of the sternum (sterno-) and the clavicle (cleido-), and has an insertion at the mastoid process of the temporal bone of the skull.
The sternocleidomastoid muscle is one of the largest and most superficial cervical muscles. The primary actions of the muscle are rotation of the head to the opposite side and flexion of the neck. The sternocleidomastoid is innervated by the accessory nerve.
It is given the name sternocleidomastoid because it originates from the top of the sternum (sterno-) and the clavicle (cleido-), and has an insertion at the mastoid process of the temporal bone of the skull.
Structure
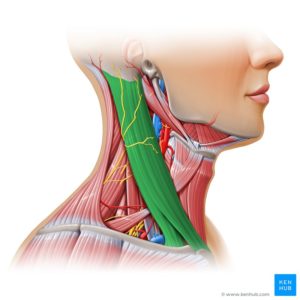
From its orignation, the SCM travels obliquely across the side of the neck and inserts on the skull. The sternocleidomastoid is thick and narrow at its centre, and broader and thinner at either end. The sternal head travels superiorly, laterally, and posteriorly, at an angle. The clavicular head is directed almost vertically upward. The two heads are separated from one another at their origins by a triangular interval but gradually blend, below the middle of the neck, into a thick, rounded muscle which is inserted, by a strong tendon, into the lateral surface of the mastoid process, from its apex to its superior border, and by a thin connection into the occipital bone.Variation
The clavicular origin of the sternocleidomastoid varies greatly: in some cases the clavicular head may be as narrow as the sternal; in others it may be as much as 7.5 millimetres (0.30 in) in breadth. When the clavicular origin is broad, it is occasionally subdivided into several slips, separated by narrow intervals. More rarely, the adjoining margins of the sternocleidomastoid and trapezius are in contact. This would leave no posterior triangle.Anatomical landmark
The sternocleidomastoid is within the investing fascia of the neck, along with the trapezius muscle, with which it shares its nerve supply (the accessory nerve). It is thick and thus serves as a primary landmark of the neck. Many important structures relate to the sternocleidomastoid, including the common carotid artery, accessory nerve, and brachial plexus.Contraction
The signaling process to contract or relax the sternocleidomastoid begins in Cranial Nerve XI, the accessory nerve. The accessory nerve nucleus is in the anterior horn of the spinal cord around C1-C3, where lower motor neuron fibers mark its origin. The fibers from the accessory nerve nucleus travel upward to enter the cranium via the foramen magnum. The trapezius is a large paired surface muscle that extends longitudinally from the occipital bone to the lower thoracic vertebrae of the spine and laterally to the spine of the scapula. It moves the scapula and supports the arm.
At its upper origin, the trapezius is connected to the bone by a thin fibrous lamina, firmly adherent to the skin. The superficial and deep epimysia are continuous with an investing deep fascia that encircles the neck and also contains both sternocleidomastoid muscles.
At the middle, the muscle is connected to the spinous processes by a broad semi-elliptical aponeurosis, which reaches from the sixth cervical to the third thoracic vertebræ and forms, with that of the opposite muscle, a tendinous ellipse. The rest of the muscle arises by numerous short tendinous fibers.
It is possible to feel the muscles of the upper trapezius become active by holding a weight in one hand in front of the body and, with the other hand, touching the area between the shoulder and the neck.
The trapezius is a large paired surface muscle that extends longitudinally from the occipital bone to the lower thoracic vertebrae of the spine and laterally to the spine of the scapula. It moves the scapula and supports the arm.
At its upper origin, the trapezius is connected to the bone by a thin fibrous lamina, firmly adherent to the skin. The superficial and deep epimysia are continuous with an investing deep fascia that encircles the neck and also contains both sternocleidomastoid muscles.
At the middle, the muscle is connected to the spinous processes by a broad semi-elliptical aponeurosis, which reaches from the sixth cervical to the third thoracic vertebræ and forms, with that of the opposite muscle, a tendinous ellipse. The rest of the muscle arises by numerous short tendinous fibers.
It is possible to feel the muscles of the upper trapezius become active by holding a weight in one hand in front of the body and, with the other hand, touching the area between the shoulder and the neck.
Nerve supply
Motor function to both the trapezius and the SCM are supplied by the accessory nerve. Sensation, including pain and the sense of joint position (proprioception), travel via the ventral rami of the third (C3) and fourth (C4) cervical nerves. Since it is a muscle of the upper limb, the trapezius is not innervated by dorsal rami despite being placed superficially in the back.Structure
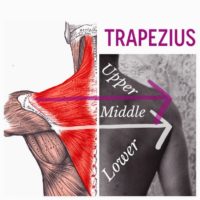 The trapezius muscle resembles a trapezium (trapezoid in American English), or diamond-shaped quadrilateral. The trapezius has three functional parts: an upper (descending) part which supports the weight of the arm; a middle region (transverse), which retracts the scapula; and a lower (ascending) part which medially rotates and depresses the scapula.
The trapezius muscle resembles a trapezium (trapezoid in American English), or diamond-shaped quadrilateral. The trapezius has three functional parts: an upper (descending) part which supports the weight of the arm; a middle region (transverse), which retracts the scapula; and a lower (ascending) part which medially rotates and depresses the scapula.
Both the trapezius and the SCM, along with their common accessory nerve originate from the same piece of embryological tissue. They are associated with feeding. Although they appear to be part of the neck and back, they are really muscles of the arm that have migrated close to the spine. They have a common evolutionary ancestor in the fossil record called the cucullaris muscle.
Function
Contraction of the trapezius muscle can have two different effects: movement of the scapulae when the spinal origins are stable, and movement of the spine when the scapulae are stable. Its main function is to stabilize and move the scapula. However, both movement of one section and stabilization against movement with another are possible at the same time or in close succession. Proper firing of these muscles as we move our arm is called scapulo-humeral rhythm.
Scapular movements
 The upper fibers elevate the scapulae, along with levator scapula. Typical actions are shrugging or hunching your shoulders. It is most active when your arms are below your shoulders.
The upper fibers elevate the scapulae, along with levator scapula. Typical actions are shrugging or hunching your shoulders. It is most active when your arms are below your shoulders.
The middle fibers retract the scapulae, along with the rhomboids. This is the action of pulling your shoulders back. It is most active when your arms are even with your shoulders.
![]() The lower fibers depress the scapulae, along with serratus anterior. This is happens when we ground our shoulders, as in a downward facing dog. It is most active when your arms are above your shoulders.
The lower fibers depress the scapulae, along with serratus anterior. This is happens when we ground our shoulders, as in a downward facing dog. It is most active when your arms are above your shoulders.
In addition to scapular translation, the trapezius induces scapular rotation. The upper and lower fibers tend to rotate the scapula around the Sternoclavicular articulation so that the acromion and inferior angles move up and the medial border moves down (upward rotation). The upper and lower fibers work in tandem with serratus anterior to upwardly rotate the scapulae, and work in opposition to the levator scapulae and the rhomboids, which effect downward rotation.
An example of trapezius function is an overhead press. When activating together, the upper and lower fibers also assist the middle fibers (along with other muscles such as the rhomboids) with scapular retraction/adduction.
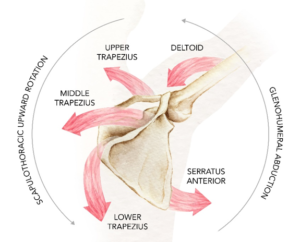
The trapezius also assists in abduction of the shoulder above 90 degrees by rotating the glenoid upward. Injury to cranial nerve XI will cause weakness in abducting the shoulder above 90 degrees.
When we have proper scapulo-humeral rhythm, the upper, middle and lower traps work together with the serratus anterior and deltoids to efficiently couple force from the body to the arm.
Spinal movements
When the scapulae are stable a co-contraction of both sides can extend the neck. A contraction of the upper trapezius from one side will flex the neck to the contracting side. It also assists in rotation of the neck.