
Hip and glute pain isn’t glamorous, but many people are living with it every day. Sometimes the pain is deep in the hip, making it difficult to lie on that side. It can also radiate down the leg to the ankle or extend to the glutes. Some refer to pain like this as ‘sciatica‘.
Gluteus Minimis
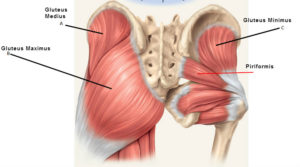 This pain is caused primarily by trigger points in the deepest and smallest of the glutes – gluteus minimus. It lies deep within the hip wrapped around the head of the femur.
This pain is caused primarily by trigger points in the deepest and smallest of the glutes – gluteus minimus. It lies deep within the hip wrapped around the head of the femur.
Tensor Fascia Latae (TFL)
The tensor fascia latae (TFL) that runs along the outside of the hip can cause a similar pain pattern. “Tensor fasciae latae” translates from Latin to English as “stretcher of the side band”.
Because it is used for so many movements and is in a shortened position when seated, the TFL becomes tight easily. TFL stretches lengthen this important muscle.
A small case notes that “it seems possible that a sloped or banked surface could predispose an individual to a TFL strain.” In such a case, “treatment usually consists of rest, heat, and flexibility exercises”, such as lliotibial band stretching.
Disc Issues
Sometimes, we see cases where lumbar disc damage is causing radiculopathy (sciatica), as well as weakness and reduced function of muscles of the leg. This can be a serious condition that should be examined by a physician.
 However, the trigger points in the glutes activated by irritation of the nerve root actually cause much of the pain of a disc injury.
However, the trigger points in the glutes activated by irritation of the nerve root actually cause much of the pain of a disc injury.
This is why patients who have had a successful microdiscectomy or similar procedure may still experience hip and glute pain after the procedure that is very similar to the original pain. These residual trigger points must be addressed for lasting pain relief.
For most of us, there is no spinal injury, just a simple activation of trigger points in a couple of key glute and hip muscles causing pain. These muscles move our leg out to the side (abduction), rotate inward at the hip and assist in flexing at the hip.
![]() To release the trigger points in your gluteus minimus and TFL, all you need is a tennis ball and bench, table or bed with a reasonably firm edge. The objective is use the tennis ball to compress the more superficial TFL and then moving toward the rear – and deeper – to reach the gluteus minimus.
To release the trigger points in your gluteus minimus and TFL, all you need is a tennis ball and bench, table or bed with a reasonably firm edge. The objective is use the tennis ball to compress the more superficial TFL and then moving toward the rear – and deeper – to reach the gluteus minimus.
We’re using the tennis ball between our glutes and the wall, searching for tender areas near the X’s on these charts. If we find them, we use the tennis ball to provide sustained, gentle pressure for 15-20 seconds. Note that the trigger points for the TFL are just in front of the mid-line of the hip. However, the referral pattern is behind that, along the femur. We do not use the tennis balls on the areas of referred pain.
Next, we want to gently stretch the gluteus minimus and TFL. For example, with glute min, this primarily means adducting the leg across the body. For the TFL, we want to extend the hip. Both muscles benefit  from rotating externally.
from rotating externally.
First, we’ll be stretching across the midline of the body (standing or passive adduction). Next, we’ll externally rotate the leg at the hip (seated glute stretch or pigeon pose) and extend the thigh at the hip (low lunge).
 For instance, from a standing posture, stretch the glute on the right side of the person as pictured. Note that the side you are stretching crosses behind the forward, planted leg. However, if you can find a bench, table or bed to lay across the passive version of this stretch works even better!
For instance, from a standing posture, stretch the glute on the right side of the person as pictured. Note that the side you are stretching crosses behind the forward, planted leg. However, if you can find a bench, table or bed to lay across the passive version of this stretch works even better!
 Next, to provide the same benefit to the posterior fibers of this muscle, the hip must be flexed. This position also provides some gentle exterior rotation to the femur at the hip. Create additional rotation by reclining and bending the straight leg to rotate the opposite leg from the ankle.
Next, to provide the same benefit to the posterior fibers of this muscle, the hip must be flexed. This position also provides some gentle exterior rotation to the femur at the hip. Create additional rotation by reclining and bending the straight leg to rotate the opposite leg from the ankle.

The TFL also benefits from these adduction and rotation stretches. However, to more fully stretch the TFL we need to put put the hip into extension. For instance, one easy way to do this is to use a basic low lunge pose. There can be a lot to think about in a low lunge; we’re focusing our attention on the extension of the long leg. More information about the TFL is in the article New Trends in IT Band Pain Relief.

Some activities can activate trigger points in these muscles. If we can avoid or modify these activities we can reduce hip and glute pain over the longer term. For example. prolonged sitting or standing immobilizes the glutes. Try using a higher chair or stool at a stand-up desk at work, opening the hips but still taking weight off the legs. When standing, consider shifting weight when standing with feet hip width apart. Use cruise control when driving long distances to free the right leg. Avoid walking or running on hills or surfaces that are sloped to one side. Avoid sleeping in the fetal position and use a thick pillow between the legs between the knee and ankle.
Self-compression is the foundation of myofascial self-care. However, in dealing with the hip and glutes, it is important to respect the different layers of muscle. Ultimately, you may need to use more pressure than in some other areas to get to the deeper layers.
If you are having similar issues, you may find that one or two treatment sessions helps identify and treat root causes of your individual case. We offer some additional treatment modalities and techniques that you may find helpful.
Issues with hip and glute pain can be complicated. They involve a significant number of muscles. Issues with the gluteus minimus and TFL usually occur as part of a complex of myofascial dysfunction. We can help sort them out.
Extra – Anatomy of Gluteus Medius and TFL
Origin and insertion
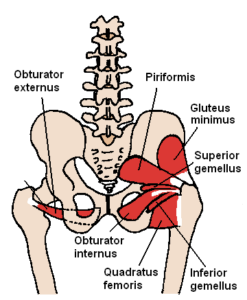
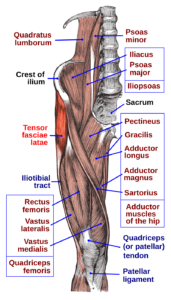
 Muscles of the gluteal and posterior femoral regions with gluteus minimus muscle highlighted.
Muscles of the gluteal and posterior femoral regions with gluteus minimus muscle highlighted.
 It is fan-shaped, arising from the outer surface of the ilium, between the anterior and inferior gluteal lines, and behind, from the margin of the greater sciatic notch.
The fibers converge to the deep surface of a radiated aponeurosis, and this ends in a tendon which is inserted into an impression on the anterior border of the greater trochanter, and gives an expansion to the capsule of the hip joint. It is also a local stabilizer for the hip.
It is fan-shaped, arising from the outer surface of the ilium, between the anterior and inferior gluteal lines, and behind, from the margin of the greater sciatic notch.
The fibers converge to the deep surface of a radiated aponeurosis, and this ends in a tendon which is inserted into an impression on the anterior border of the greater trochanter, and gives an expansion to the capsule of the hip joint. It is also a local stabilizer for the hip.
Relations
A bursa is interposed between the tendon and the greater trochanter. Between the gluteus medius and gluteus minimus are the deep branches of the superior gluteal vessels and the superior gluteal nerve. The deep surface of the gluteus minimus is in relation with the reflected tendon of the rectus femoris and the capsule of the hip joint.Variations
The muscle may be divided into an anterior and a posterior part, or it may send slips to the piriformis, the superior gemellus or the outer part of the origin of the vastus lateralis.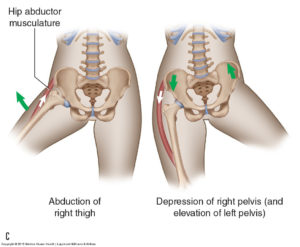 The gluteus medius and gluteus minimus abduct the thigh, when the limb is extended, and are principally called into action in supporting the body on one limb, in conjunction with the tensor fasciæ latæ.
Their anterior fibers also flex the hip, and by drawing the greater trochanter forward, rotate the thigh inward, in which action they are also assisted by the tensor fasciæ latæ.
Additionally, with the hip flexed, the gluteus medius and minimus internally rotate the thigh. With the hip extended, the gluteus medius and gluteus minimus externally rotate the thigh.
The attachment to the superior capsule of the hip may also serve to retract the capsule away from the joint during motion. This mechanism may prevent capsular impingement similar to the role of the articularis genus in the knee.
The gluteus medius and gluteus minimus abduct the thigh, when the limb is extended, and are principally called into action in supporting the body on one limb, in conjunction with the tensor fasciæ latæ.
Their anterior fibers also flex the hip, and by drawing the greater trochanter forward, rotate the thigh inward, in which action they are also assisted by the tensor fasciæ latæ.
Additionally, with the hip flexed, the gluteus medius and minimus internally rotate the thigh. With the hip extended, the gluteus medius and gluteus minimus externally rotate the thigh.
The attachment to the superior capsule of the hip may also serve to retract the capsule away from the joint during motion. This mechanism may prevent capsular impingement similar to the role of the articularis genus in the knee.
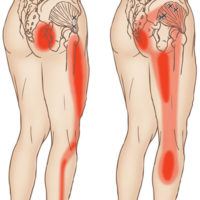 Trigger points in your gluteus minimus can cause significant hip pain. This can cause difficulty bearing weight on the affected side and lead to a limp.
It may be painful when you are walking, lying down or trying to get up from sitting. Pain can be constant and excruciating. You may have pain when trying to lie on the affected side, making it necessary to switch to the other side.
You may not be able to find a position to lie down comfortably or walk normally. It is also painful to stand for an extended time. You may try to shift weight from leg to another to avoid pain in your hip and leg.
It is difficult to find a stretch or other movement that that relieves the pain.
Trigger points in your gluteus minimus can cause significant hip pain. This can cause difficulty bearing weight on the affected side and lead to a limp.
It may be painful when you are walking, lying down or trying to get up from sitting. Pain can be constant and excruciating. You may have pain when trying to lie on the affected side, making it necessary to switch to the other side.
You may not be able to find a position to lie down comfortably or walk normally. It is also painful to stand for an extended time. You may try to shift weight from leg to another to avoid pain in your hip and leg.
It is difficult to find a stretch or other movement that that relieves the pain.
 Gluteus minimus is active throughout the stance phase of your gait. This is why changes in the mechanices of how you walk or run can activate or perpetuate gluteus minimus trigger points.
The demand on gluteus minimus is increased when chronic increased adduction at the hip occurs. Than can be caused by an injury to another joint, genu valgus (knock knee-ed), pronation of your feet or weakness of the other abductors of the hip, including gluteus maximus and and medius, TFL, piriformic, the obturators and gemelli.
Trigger points can also be activated by overload from a fall. In addition, unconditioned overuse from running, racquet sports or hiking over uneven ground overload the gluteus minimus and activate TrPs. Standing or sitting for prolonged periods of time can aggravate the gluteus minimus, especially sitting on a wallet or uneven surface.
Lumbar radiculopathy from L4,L5 or S1 frequently induce spasms and activate trigger points in gluteus minimus. Treatment of these TrPs will only provide limited relief until the nerve root inflammation is reduced. Although residual TrPs may remain, treatment of these is likely to provide lasting relief.
Gluteus minimus is active throughout the stance phase of your gait. This is why changes in the mechanices of how you walk or run can activate or perpetuate gluteus minimus trigger points.
The demand on gluteus minimus is increased when chronic increased adduction at the hip occurs. Than can be caused by an injury to another joint, genu valgus (knock knee-ed), pronation of your feet or weakness of the other abductors of the hip, including gluteus maximus and and medius, TFL, piriformic, the obturators and gemelli.
Trigger points can also be activated by overload from a fall. In addition, unconditioned overuse from running, racquet sports or hiking over uneven ground overload the gluteus minimus and activate TrPs. Standing or sitting for prolonged periods of time can aggravate the gluteus minimus, especially sitting on a wallet or uneven surface.
Lumbar radiculopathy from L4,L5 or S1 frequently induce spasms and activate trigger points in gluteus minimus. Treatment of these TrPs will only provide limited relief until the nerve root inflammation is reduced. Although residual TrPs may remain, treatment of these is likely to provide lasting relief.
Structure
 It arises from the anterior part of the outer lip of the iliac crest; from the outer surface of the anterior superior iliac spine, and part of the outer border of the notch below it, between the gluteus medius and sartorius; and from the deep surface of the fascia lata.
It is inserted between the two layers of the iliotibial tract of the fascia lata about the junction of the middle and upper thirds of the thigh. The tensor fasciae latae tautens the iliotibial tract and braces the knee, especially when the opposite foot is lifted. The terminal insertion point lies as far as the lateral condyle of the tibia.
It arises from the anterior part of the outer lip of the iliac crest; from the outer surface of the anterior superior iliac spine, and part of the outer border of the notch below it, between the gluteus medius and sartorius; and from the deep surface of the fascia lata.
It is inserted between the two layers of the iliotibial tract of the fascia lata about the junction of the middle and upper thirds of the thigh. The tensor fasciae latae tautens the iliotibial tract and braces the knee, especially when the opposite foot is lifted. The terminal insertion point lies as far as the lateral condyle of the tibia.
Nerve supply
Tensor fasciae latae is innervated by the superior gluteal nerve, L5 and S1. At its origins of the anterior rami of L4, L5, and S1 nerves, the superior gluteal nerve exits the pelvis via greater sciatic foramen superior to the piriformis. The nerve also courses between the gluteus medius and minimus. The superior gluteal artery also supplies the tensor fasciae latae.[1] The superior gluteal nerve arises from the sacral plexus and only has muscular innervation associated with it. There is no cutaneous innervation for sensation that stems from the superior gluteal nerve.[2]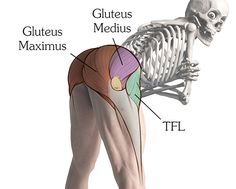 Trigger points in the TFL can be caused by sudden trauma, such as landing on from high jump. More often if comes from chronic overload, such as jogging up and down hill without support for a pronated foot.
In general, extended walking or running on uneven surfaces can activate tensor fascia latae TrPs because they force one foot into pronation and the other into supination and have a compensatory effect on your knees and hips.
Poor conditioning and inadequate warmups can lead to injuries that activate or perpetuate TrPs in the TFL muscle. Weakness or inhibition of the gluteus medius or gluteus minimus can cause overload of the TFL because they act together to stabilize the hip.
As with other muscles, the tensor fascia latae are aggravated by immobilization in the shortened position for extended periods of time. For example, this happens during prolonged sitting or sleeping on your side with your hips tightly flexed. Walking with heavy loads can also overload this muscle.
Trigger points in the TFL can be caused by sudden trauma, such as landing on from high jump. More often if comes from chronic overload, such as jogging up and down hill without support for a pronated foot.
In general, extended walking or running on uneven surfaces can activate tensor fascia latae TrPs because they force one foot into pronation and the other into supination and have a compensatory effect on your knees and hips.
Poor conditioning and inadequate warmups can lead to injuries that activate or perpetuate TrPs in the TFL muscle. Weakness or inhibition of the gluteus medius or gluteus minimus can cause overload of the TFL because they act together to stabilize the hip.
As with other muscles, the tensor fascia latae are aggravated by immobilization in the shortened position for extended periods of time. For example, this happens during prolonged sitting or sleeping on your side with your hips tightly flexed. Walking with heavy loads can also overload this muscle.