 The supraspinatus muscle is the most active of the four rotator cuff muscles. It is responsible for abduction of the your arm at the shoulder. Most importantly, in conjunction with the other rotator cuff muscles, it is responsible for dynamic stabilization of the shoulder joint.
The supraspinatus muscle is the most active of the four rotator cuff muscles. It is responsible for abduction of the your arm at the shoulder. Most importantly, in conjunction with the other rotator cuff muscles, it is responsible for dynamic stabilization of the shoulder joint.
The shoulder has less connective tissue structure than other major joints. The rotator cuff muscles act as a sort of dynamic muscle/ligament hybrid to stabilize the shoulder joint as you move.
Of the important functions of supraspinatus is to provide resistance against the downward migration of your humerus during the arm swing of normal gait.
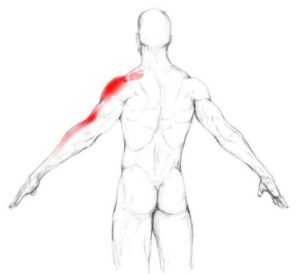
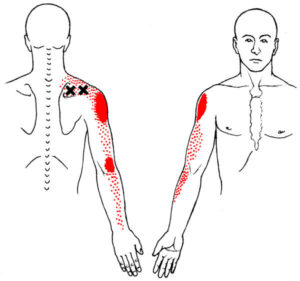
Trigger points in your supraspinatus cause pain on the side of the shoulder, and sometimes extending down the side of your arm to the elbow and forearm.
Supraspinatus trigger points are often involved with shoulder impingement syndromes. It is also the most frequently torn rotator cuff muscle.
 The supraspinatus muscle is a common source of shoulder pain. In individuals with non-specific shoulder pain 38% had supraspinatus trigger points. For patients diagnosed with a shoulder impingement rate was even higher - 65%!
Supraspinatus TrPs is typically cause intense on the outside of the of your shoulder, over the deltoids. Pain can spread down the arm past the elbow and to the forearm.
You will probably feel the pain most intensely when raising (abducting) your arm at the shoulder, especially as you being the movement. The pain may prevent you from getting your arm over your head.
If the supraspinatus on your dominant side is affected, you may have difficulty with reaching your head to comb or brush your hair, brush your teeth, apply makeup or shave facial hair. However, if the trigger points are on your non-dominant side, you may not notice even moderate restrictions unless you make movements that are unusual for you.
You may have deep ache on the outside of the shoulder at rest that is similar to bursitis.
If the supraspinatus is highly irritated, you may have shoulder pain when walking due to activation of the muscle during arm swing.
Supraspinatus trigger points should be suspected if you have recurring lateral elbow pain, also known as 'tennis elbow' or lateral epicondylalgia.
Supraspinatus trigger points alone rarely cause severe, sleep disturbing pain. In patients over 65 with pain that disturbs sleep, an examination for a rotator cuff tear should be performed.
Popping or clicking sounds near the shoulder may be due to supraspinatus trigger points that resolve when treated.
The supraspinatus muscle is a common source of shoulder pain. In individuals with non-specific shoulder pain 38% had supraspinatus trigger points. For patients diagnosed with a shoulder impingement rate was even higher - 65%!
Supraspinatus TrPs is typically cause intense on the outside of the of your shoulder, over the deltoids. Pain can spread down the arm past the elbow and to the forearm.
You will probably feel the pain most intensely when raising (abducting) your arm at the shoulder, especially as you being the movement. The pain may prevent you from getting your arm over your head.
If the supraspinatus on your dominant side is affected, you may have difficulty with reaching your head to comb or brush your hair, brush your teeth, apply makeup or shave facial hair. However, if the trigger points are on your non-dominant side, you may not notice even moderate restrictions unless you make movements that are unusual for you.
You may have deep ache on the outside of the shoulder at rest that is similar to bursitis.
If the supraspinatus is highly irritated, you may have shoulder pain when walking due to activation of the muscle during arm swing.
Supraspinatus trigger points should be suspected if you have recurring lateral elbow pain, also known as 'tennis elbow' or lateral epicondylalgia.
Supraspinatus trigger points alone rarely cause severe, sleep disturbing pain. In patients over 65 with pain that disturbs sleep, an examination for a rotator cuff tear should be performed.
Popping or clicking sounds near the shoulder may be due to supraspinatus trigger points that resolve when treated.
 When a posture or activity that activates a trigger point is not corrected, it can also perpetuate it. Trigger points can be activated anywhere in the supraspinatus from unaccustomed eccentric loading, eccentric exercise in an unconditioned muscle, maximal or sub-maximal concentric loading.
Placing the muscle in a shortened or lengthened position for an extended period of time can also activate trigger points in the supraspinatus.
When a posture or activity that activates a trigger point is not corrected, it can also perpetuate it. Trigger points can be activated anywhere in the supraspinatus from unaccustomed eccentric loading, eccentric exercise in an unconditioned muscle, maximal or sub-maximal concentric loading.
Placing the muscle in a shortened or lengthened position for an extended period of time can also activate trigger points in the supraspinatus.
 Activies that can overload your supraspinatus include carrying heavy items such a suitcase, briefcase or tool bag with your arm hanging down.
This can also happen from regularly walking a large dog that pulls on the leash.
Another common cause of supraspinatus TrP activations is an object to shoulder height or above with your arm outstretched.
Finally, activities that involve repeated elevation or prolonged elevation of your arm, especially from the side, can activate the supraspinatus. An example would be holding a phone up to your ear, elevating your arm (abducting it) from the side, bagging groceries, and certain swimming strokes.
Activies that can overload your supraspinatus include carrying heavy items such a suitcase, briefcase or tool bag with your arm hanging down.
This can also happen from regularly walking a large dog that pulls on the leash.
Another common cause of supraspinatus TrP activations is an object to shoulder height or above with your arm outstretched.
Finally, activities that involve repeated elevation or prolonged elevation of your arm, especially from the side, can activate the supraspinatus. An example would be holding a phone up to your ear, elevating your arm (abducting it) from the side, bagging groceries, and certain swimming strokes.
 It is fairly difficult to find an angle that will allow you to use a tennis or lacrosse ball effectively on supraspinatus. Instead, you can release supraspinatus trigger points yourself using a tool such as the Back Knobber. The problem with this illustration is that the affected arm is raised. It is good to move the arm through its range of motion during self-compression. However, it is best to let your arm rest at your side during this manuever.
It is fairly difficult to find an angle that will allow you to use a tennis or lacrosse ball effectively on supraspinatus. Instead, you can release supraspinatus trigger points yourself using a tool such as the Back Knobber. The problem with this illustration is that the affected arm is raised. It is good to move the arm through its range of motion during self-compression. However, it is best to let your arm rest at your side during this manuever.
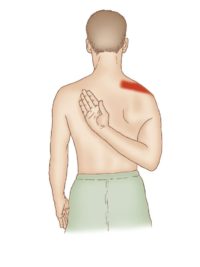 A more aggresive approach involves adducting and internally rotating your arm behind your back. With each exhalation, let the muscle relax and see if you can reach up a little further.
A more aggresive approach involves adducting and internally rotating your arm behind your back. With each exhalation, let the muscle relax and see if you can reach up a little further.
 You can deepen this stretch by using reciprocal inhibition to activate the antagonists of the supraspinatus.
You can repeat this sequence three to five times, up to four times per day.
Following pressure release or stretching a cold pack may be helpful.
If tightness of the posterior capsule develops it is essential that the connective tissue function with the joint be addressed in addition to restoring normal mechanics of your arm and shoulder while treating trigger points in the supraspinatus. If treatment is limited to this individual muscle without addressing the mechanics of the entire joint will fail and pain relief will be temporary.
You can deepen this stretch by using reciprocal inhibition to activate the antagonists of the supraspinatus.
You can repeat this sequence three to five times, up to four times per day.
Following pressure release or stretching a cold pack may be helpful.
If tightness of the posterior capsule develops it is essential that the connective tissue function with the joint be addressed in addition to restoring normal mechanics of your arm and shoulder while treating trigger points in the supraspinatus. If treatment is limited to this individual muscle without addressing the mechanics of the entire joint will fail and pain relief will be temporary.
 Avoid sustained or repetitive actions that overload the supraspinatus muscle such as carrying heavy items hanging down at your side. However you should also avoid lifting heavy objects overhead, backward or out to the side. Avoid wearing backpack that exerts sustained pressure on these muscles.
Avoid sustained contraction of the supraspinatus. For example, 20 minutes or more of hairstyling or work overhead can easily activate this muscle. Take short breaks so give the supraspinatus a chance to recover.
Avoid sustained or repetitive actions that overload the supraspinatus muscle such as carrying heavy items hanging down at your side. However you should also avoid lifting heavy objects overhead, backward or out to the side. Avoid wearing backpack that exerts sustained pressure on these muscles.
Avoid sustained contraction of the supraspinatus. For example, 20 minutes or more of hairstyling or work overhead can easily activate this muscle. Take short breaks so give the supraspinatus a chance to recover.
 Restful sleep may be difficult due to pain. Consider sleeping on your back or on the uninvolved side. If you sleep on the pain-free side your sleep will be improved if you support the painful arm on a pillow, avoiding the prolonged lengthening that can lead to pain.
Restful sleep may be difficult due to pain. Consider sleeping on your back or on the uninvolved side. If you sleep on the pain-free side your sleep will be improved if you support the painful arm on a pillow, avoiding the prolonged lengthening that can lead to pain.
 You can also use this technique to support the painful arm when sleeping on your back or when sitting.
In general, do not sleep on your stomach. Do not lie on either on your back with your arms extended up over your head. This will externally rotate your arms and keep the supraspinatus in a shortened position for an extended time.
You can also use this technique to support the painful arm when sleeping on your back or when sitting.
In general, do not sleep on your stomach. Do not lie on either on your back with your arms extended up over your head. This will externally rotate your arms and keep the supraspinatus in a shortened position for an extended time.
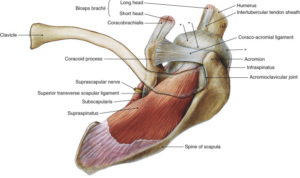
 Supraspinatus, along with infrapinatus, teres minor, and subscapularis insert into the lesser and greater tuberosities on the front and back of your humerus. They form a 'cuff' of connnective tissue and muscles around the head of your humerus that help rotate your arm at the shoulder. Collectively, they are called the rotator cuff. The supraspinatus muscle is the most active rotator cuff muscle and is involved in almost anything you do that involves raising your arm.
Supraspinatus, along with infrapinatus, teres minor, and subscapularis insert into the lesser and greater tuberosities on the front and back of your humerus. They form a 'cuff' of connnective tissue and muscles around the head of your humerus that help rotate your arm at the shoulder. Collectively, they are called the rotator cuff. The supraspinatus muscle is the most active rotator cuff muscle and is involved in almost anything you do that involves raising your arm.
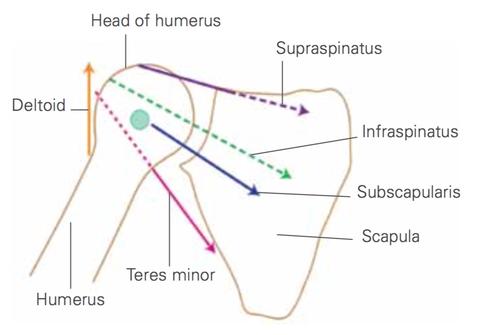 Although each of these rotator cuff muscles participate in the rotation of your arm, their primary purpose is to pull the head of humerus fairly tight into the shallow socket of the shoulder blade. Unlike your knee or ankle, this stability is created by largely these rotator cuff muscles, not ligaments. It part of what allows us to have much greater range of motion at our shoulder than any other joint. For this stabilizing function, you could think of them as powered, dynamic ligaments.
Of the rotator cuff muscles, supraspinatus is the most active during the early phases of abduction of your arm.
Although each of these rotator cuff muscles participate in the rotation of your arm, their primary purpose is to pull the head of humerus fairly tight into the shallow socket of the shoulder blade. Unlike your knee or ankle, this stability is created by largely these rotator cuff muscles, not ligaments. It part of what allows us to have much greater range of motion at our shoulder than any other joint. For this stabilizing function, you could think of them as powered, dynamic ligaments.
Of the rotator cuff muscles, supraspinatus is the most active during the early phases of abduction of your arm. 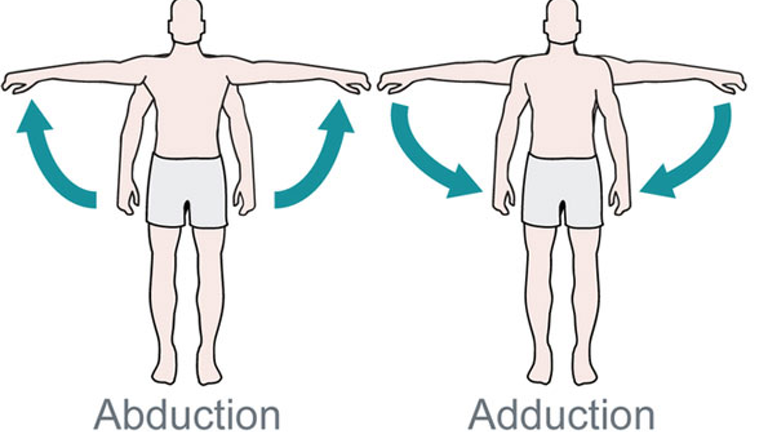 The other muscles activate more strongly later in the movement. Individually, the certain rotator muscles are recruited early and different muscles activate later, keeping the head of the humerus stable in most movements.
In both abduction and flexion, elevating the arm to 90 degrees, the supraspinatus fatigues before any other muscle in the shoulder girdle. Workers who need to maintain their arms in an elevated position have a high incidence of supraspinatus tendonopathy. This is imporant when driving. Adjusting your seat closer to the steering wheel allows your shoulders to rest and reduces average supraspinatus activity by 45%.
Supraspinatus is active during the forward and backward arm swing as part of our gait. However, its primary action is counter the downward pull of the humerus as we walk.
The other muscles activate more strongly later in the movement. Individually, the certain rotator muscles are recruited early and different muscles activate later, keeping the head of the humerus stable in most movements.
In both abduction and flexion, elevating the arm to 90 degrees, the supraspinatus fatigues before any other muscle in the shoulder girdle. Workers who need to maintain their arms in an elevated position have a high incidence of supraspinatus tendonopathy. This is imporant when driving. Adjusting your seat closer to the steering wheel allows your shoulders to rest and reduces average supraspinatus activity by 45%.
Supraspinatus is active during the forward and backward arm swing as part of our gait. However, its primary action is counter the downward pull of the humerus as we walk.
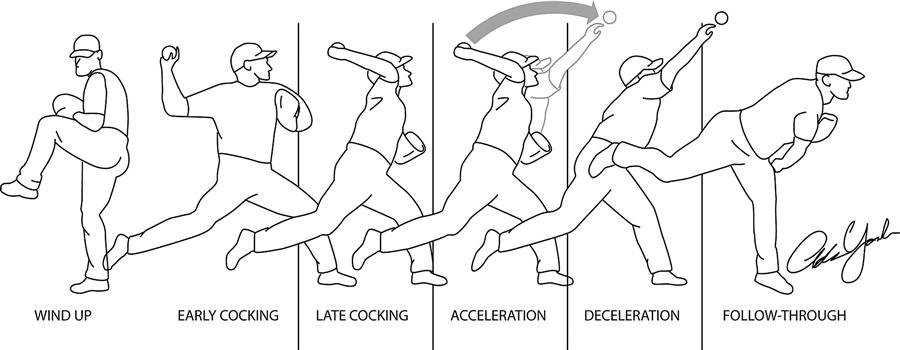 During a throwing motion, supraspinatus is most active during the early and late cocking phases of the throw. Less experienced players tend to using supraspinatus more during the acceleration phase of the movement. The supraspinatus also activates eccentrically to decelerate the arm when throwing.
During a golf swing, activity in the dominant shoulder starts at a moderate level and decreases to about 10% by late follow through. The non-dominant side maintains moderate activity throughout the swing, with more during early and late follow through.
During a throwing motion, supraspinatus is most active during the early and late cocking phases of the throw. Less experienced players tend to using supraspinatus more during the acceleration phase of the movement. The supraspinatus also activates eccentrically to decelerate the arm when throwing.
During a golf swing, activity in the dominant shoulder starts at a moderate level and decreases to about 10% by late follow through. The non-dominant side maintains moderate activity throughout the swing, with more during early and late follow through.
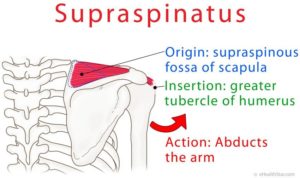
 The supraspinatus is a relatively small muscle of the upper back that runs from the supraspinous fossa superior portion of the scapula (shoulder blade) to the greater tubercle of the humerus. It is one of the four rotator cuff muscles and also abducts the arm at the shoulder. The spine of the scapula separates the supraspinatus muscle from the infraspinatus muscle, which originates below the spine.
The supraspinatus is a relatively small muscle of the upper back that runs from the supraspinous fossa superior portion of the scapula (shoulder blade) to the greater tubercle of the humerus. It is one of the four rotator cuff muscles and also abducts the arm at the shoulder. The spine of the scapula separates the supraspinatus muscle from the infraspinatus muscle, which originates below the spine.
Structure
The supraspinatus muscle arises from the supraspinous fossa, a shallow depression in the body of the scapula above its spine and the supraspinous fascia. It is thinner towards the spine and becomes thicker towards the shoulder.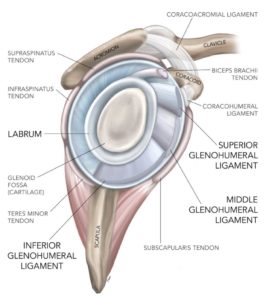 The fibers of the front side of supraspinatus are angled obliquely but the fibers on the back side of the muscle are more straight. This facilitates the multiple actions of supraspinatus. These two sections converge to form a thick tendon under the acromion of the shoulder blade. This narrow passage is one of the trouble spots for supraspinatus.
The fibers of the front side of supraspinatus are angled obliquely but the fibers on the back side of the muscle are more straight. This facilitates the multiple actions of supraspinatus. These two sections converge to form a thick tendon under the acromion of the shoulder blade. This narrow passage is one of the trouble spots for supraspinatus.
Relations
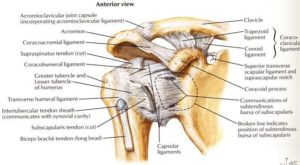 As the tendon continues, it passes over the head of the humerus and inserts onto the greater tubercle. The tendon is thicker at the front side of its attachment and is interweaves with the tendons of subscapularis, infraspinatus and the pectoral fascia to form the transverse and coracohumeral ligaments. The tendon is flatter at its upper attachment and the deeper portion blends with the joint capsule. Recent research shows that the origin from the rear is more lateral than classically described.
As the tendon continues, it passes over the head of the humerus and inserts onto the greater tubercle. The tendon is thicker at the front side of its attachment and is interweaves with the tendons of subscapularis, infraspinatus and the pectoral fascia to form the transverse and coracohumeral ligaments. The tendon is flatter at its upper attachment and the deeper portion blends with the joint capsule. Recent research shows that the origin from the rear is more lateral than classically described.
 The supraspinatus muscle has three distinct heads that weave together to form the supraspinatus tendon. The head on the front side passes to the back, the head in the middle passes straight across and the head in the back passes to the front side. The thinner rear rear tendon overlaps the front and middle heads. This intertwines all three heads and increases the tensile capacity of the tendon.
In about 50% of the population an overgrowth of connective tissue called an aponeurotic expansion continues from the beneath the supraspinatus tendon parallel to the long head of the biceps tendon in the biciptal groove. This is outside the tendon sheath and inserts into the humerus at the top of the pectoralis major tendon.
The supraspinatus muscle has three distinct heads that weave together to form the supraspinatus tendon. The head on the front side passes to the back, the head in the middle passes straight across and the head in the back passes to the front side. The thinner rear rear tendon overlaps the front and middle heads. This intertwines all three heads and increases the tensile capacity of the tendon.
In about 50% of the population an overgrowth of connective tissue called an aponeurotic expansion continues from the beneath the supraspinatus tendon parallel to the long head of the biceps tendon in the biciptal groove. This is outside the tendon sheath and inserts into the humerus at the top of the pectoralis major tendon.
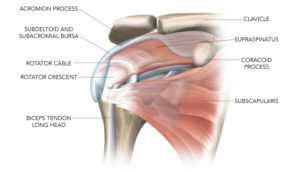 Passing towards the shoulder joint from the infraspinatus muscle, deeper vertical fibers merge with the top of the supraspinatus tendon and cross the rotator cuff interval. These extend all the way to the biceps brachii muscle itself. This thick, fibrous tendon is called the rotator cable. It links the rotator cuff muscles in the back with the muscles on the front.
Passing towards the shoulder joint from the infraspinatus muscle, deeper vertical fibers merge with the top of the supraspinatus tendon and cross the rotator cuff interval. These extend all the way to the biceps brachii muscle itself. This thick, fibrous tendon is called the rotator cable. It links the rotator cuff muscles in the back with the muscles on the front.
 The rotator crescent is the terminal connection of the supraspinatus and infraspinatus tendons that inserts onto the humerus next to the rotator cable. The rotator cable protects the rotator crescent by intrinsically transferring forces from the rear side of the rotator cuff to the front. This complicated arrangement allows the rotator cuff to work in a coordinated way no matter how your shoulder moves.
The rotator crescent is the terminal connection of the supraspinatus and infraspinatus tendons that inserts onto the humerus next to the rotator cable. The rotator cable protects the rotator crescent by intrinsically transferring forces from the rear side of the rotator cuff to the front. This complicated arrangement allows the rotator cuff to work in a coordinated way no matter how your shoulder moves.
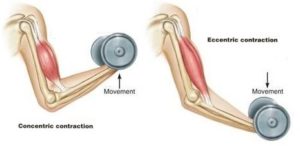 For example, in a biceps curl, you would use a concentric contraction of your biceps, coupled with an eccentric contraction of your triceps, to flex your elbow and push the weight up. As you lower the weight, eccentric contractions of your biceps are required to maintain control and prevent dropping the weight.
For example, in a biceps curl, you would use a concentric contraction of your biceps, coupled with an eccentric contraction of your triceps, to flex your elbow and push the weight up. As you lower the weight, eccentric contractions of your biceps are required to maintain control and prevent dropping the weight.
Isotonic Contractions
Isotonic contractions maintain constant tension in the muscle as the muscle changes length. This can occur only when a muscle’s maximal force of contraction exceeds the total load on the muscle. Isotonic muscle contractions can be either concentric (muscle shortens) or eccentric (muscle lengthens).Concentric Contractions
A concentric contraction is a type of muscle contraction in which the muscle shortens while generating force. This is typical of muscles that contract due to the sliding filament mechanism, and it occurs throughout the muscle. Such contractions also alter the angle of the joints to which the muscles are attached.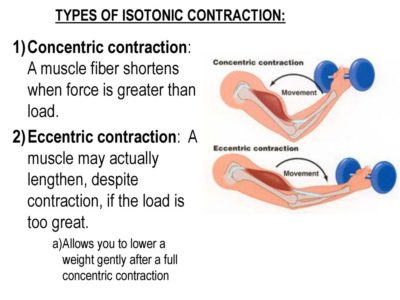 This occurs throughout the length of the muscle, generating force; causing the muscle to shorten and the angle of the joint to change. For instance, a concentric contraction of the biceps would cause the arm to bend at the elbow as the hand moves close to the shoulder (a biceps curl).
A concentric contraction of the triceps would change the angle of the joint in the opposite direction, straightening the arm and moving the hand away from the shoulder.
This occurs throughout the length of the muscle, generating force; causing the muscle to shorten and the angle of the joint to change. For instance, a concentric contraction of the biceps would cause the arm to bend at the elbow as the hand moves close to the shoulder (a biceps curl).
A concentric contraction of the triceps would change the angle of the joint in the opposite direction, straightening the arm and moving the hand away from the shoulder.
Eccentric Contractions
An eccentric contraction results in the lengthening of a muscle. These contractions decelerate muscles and joints (acting as “brakes” to concentric contractions) and can alter the position of the load force. During an eccentric contraction, the muscle lengthens while under tension due to an opposing force that is greater than the force generated by the muscle. However, rather than working to pull a joint in the direction of the muscle contraction, the muscle acts to decelerate the joint at the end of a movement or otherwise control the repositioning of a load. This can occur involuntarily (when attempting to move a weight too heavy for the muscle to lift) or voluntarily (when the muscle is “smoothing out” a movement). Strength training involving both eccentric and concentric contractions appears to increase muscular strength and joint stability more than training with concentric contractions alone.Isometric Contractions
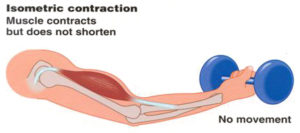 In contrast to isotonic contractions, isometric contractions generate force without changing the length of the muscle. This is typical of muscles found in the hands and forearm: the muscles do not change length, and joints are not moved, so force for grip is sufficient. An example is when the muscles of the hand and forearm grip an object; the joints of the hand do not move, but muscles generate sufficient force to prevent the object from being dropped.
For people with hypermobile joints, strength training can be a challenge. Tension stresses the connective tissues of the joint as force is transmitted through its range of motion. Isometric exercises can be ideal in these circumstances because there is minimal movement. This means that the joint is placed into vulnerable hyperextended positions under force.
In contrast to isotonic contractions, isometric contractions generate force without changing the length of the muscle. This is typical of muscles found in the hands and forearm: the muscles do not change length, and joints are not moved, so force for grip is sufficient. An example is when the muscles of the hand and forearm grip an object; the joints of the hand do not move, but muscles generate sufficient force to prevent the object from being dropped.
For people with hypermobile joints, strength training can be a challenge. Tension stresses the connective tissues of the joint as force is transmitted through its range of motion. Isometric exercises can be ideal in these circumstances because there is minimal movement. This means that the joint is placed into vulnerable hyperextended positions under force. You can develop amazing strength without free weights, machines, or resistance bands.
One of the original bodybuilder gurus from the 1920s, Charles Atlas, based his workouts primarily on isometric exercises, eventually even trademarking a term for his exercise method that he called "Dynamic Tension."
If you have hypermobile joints you can strength train safely at home with isometric exercises.
You can develop amazing strength without free weights, machines, or resistance bands.
One of the original bodybuilder gurus from the 1920s, Charles Atlas, based his workouts primarily on isometric exercises, eventually even trademarking a term for his exercise method that he called "Dynamic Tension."
If you have hypermobile joints you can strength train safely at home with isometric exercises.