Teres minor is a small, rounded rotator cuff muscle. It is the smallest of the four. It attaches from the rear, outer edge of the shoulder blade to the head of the humerus. Most importantly, in conjunction with the other rotator cuff muscles, it is responsible for dynamic stabilization of the shoulder joint, especially during upward movement of your arm.
Teres minor is a small, rounded rotator cuff muscle. It is the smallest of the four. It attaches from the rear, outer edge of the shoulder blade to the head of the humerus. Most importantly, in conjunction with the other rotator cuff muscles, it is responsible for dynamic stabilization of the shoulder joint, especially during upward movement of your arm.
The shoulder has less connective tissue structure than other major joints. The rotator cuff muscles, including teres minor, act as a sort of dynamic muscle/ligament hybrid to stabilize your shoulder joint as you move.
The other important function of teres minor is to provide externally rotate your arm.
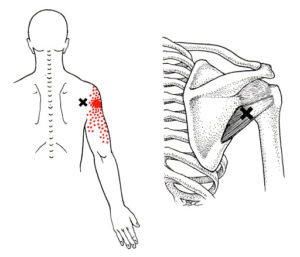
Trigger points in your teres minor refer pain deep in the back part of the deltoid area and can extend down your arm.
Teres minor trigger points are activated by overload reaching backward or upward. Corrective actions include behavior change to reduce overload, self-pressure release and stretching exercises.
 Teres minor trigger points are found in about 45% of individuals with non-specific shoulder pain. However, compared to the other rotator cuff muscles teres minor is less involved with primary shoulder pain disorders.
Teres minor trigger points are found in about 45% of individuals with non-specific shoulder pain. However, compared to the other rotator cuff muscles teres minor is less involved with primary shoulder pain disorders.
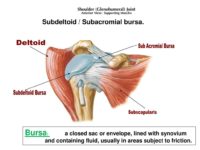 Trigger points in the teres minor often cause pain deep in beneath the deltoid in the rear. You may even get diagnosed with a painful bursa because of the spot tenderness. However, not everyone has a subacromial bursa and teres minor communicates poorly with the bursa in this area.
You are more likely to be concerned about pain in the back of your shoulder than limited range of motion. However, since trigger points in teres minor often occur along with infraspinatus, you may initial have pain in the front of your shoulder. Once the infraspinatus trigger points are eliminated, you are more likely to notice the pain the back of your shoulder caused by teres minor.
Sometimes, pain and tingling from teres minor trigger points can extend into the fourth and fifth fingers of your hand. The symptoms were aggravated by reaching up or behind the shoulder.
Trigger points in the teres minor often cause pain deep in beneath the deltoid in the rear. You may even get diagnosed with a painful bursa because of the spot tenderness. However, not everyone has a subacromial bursa and teres minor communicates poorly with the bursa in this area.
You are more likely to be concerned about pain in the back of your shoulder than limited range of motion. However, since trigger points in teres minor often occur along with infraspinatus, you may initial have pain in the front of your shoulder. Once the infraspinatus trigger points are eliminated, you are more likely to notice the pain the back of your shoulder caused by teres minor.
Sometimes, pain and tingling from teres minor trigger points can extend into the fourth and fifth fingers of your hand. The symptoms were aggravated by reaching up or behind the shoulder.
 When a posture or activity that activates a trigger point is not corrected, it can also perpetuate it. Trigger points can be activated anywhere in the teres minor from unaccustomed eccentric loading, eccentric exercise in an unconditioned muscle, maximal or sub-maximal concentric loading.
Placing the muscle in a shortened or lengthened position for an extended period of time can also activate trigger points in the teres minor muscle.
Teres minor is activated by many of the same activities and conditions that as infraspinatus trigger points. It is most often activated by major acute or minor repetitive overload. For instance, frequently reaching to the back seat of a car to tend to an young child is a repeated minor overload.
When a posture or activity that activates a trigger point is not corrected, it can also perpetuate it. Trigger points can be activated anywhere in the teres minor from unaccustomed eccentric loading, eccentric exercise in an unconditioned muscle, maximal or sub-maximal concentric loading.
Placing the muscle in a shortened or lengthened position for an extended period of time can also activate trigger points in the teres minor muscle.
Teres minor is activated by many of the same activities and conditions that as infraspinatus trigger points. It is most often activated by major acute or minor repetitive overload. For instance, frequently reaching to the back seat of a car to tend to an young child is a repeated minor overload.
 Losing your balance going down the stairs and suddenly reaching back for the railing is a more significant acute overload. Vigorous weight training with heavy overhead loads is a continued, but acute overload. A moving vehicle accident can cause teres minor trigger points, regardless of the direction of impact, especially for the driver, holding on to the steering wheel.
Other examples of acute overload include losing your balance with a heavy item overhead, working in cramped quarters with your arms overhead, a hard tennis serve delivered when slightly off balance or playing overhead sports competively.
Losing your balance going down the stairs and suddenly reaching back for the railing is a more significant acute overload. Vigorous weight training with heavy overhead loads is a continued, but acute overload. A moving vehicle accident can cause teres minor trigger points, regardless of the direction of impact, especially for the driver, holding on to the steering wheel.
Other examples of acute overload include losing your balance with a heavy item overhead, working in cramped quarters with your arms overhead, a hard tennis serve delivered when slightly off balance or playing overhead sports competively.
 The teres minor muscle can be access easily with a tennis or lacrosse ball. In addition, for more precise location of trigger points you can release teres minor yourself using a tool such as the Back Knobber. The location is a bit different from the infraspinatus, despite similarity in perpetuating factors.
The teres minor muscle can be access easily with a tennis or lacrosse ball. In addition, for more precise location of trigger points you can release teres minor yourself using a tool such as the Back Knobber. The location is a bit different from the infraspinatus, despite similarity in perpetuating factors.
 You may also find that it work well to use this tool laying down. This allows the entire shoulder girdle to relax as you treat the teres minor and other muscles. You can roll into from this position flat on your back.
Maintain increasing pressure for one to two minutes. This self-release can be repeated several times a day until the trigger points are inactivated.
You may also find that it work well to use this tool laying down. This allows the entire shoulder girdle to relax as you treat the teres minor and other muscles. You can roll into from this position flat on your back.
Maintain increasing pressure for one to two minutes. This self-release can be repeated several times a day until the trigger points are inactivated.
 You can also stretch the teres minor in similarly to infraspinatus but you may feel it differently.
You can deepen this stretch by using reciprocal inhibition to activate the antagonists of the infraspinatus and teres minor.
Following pressure release or stretching a cold pack may be helpful.
If tightness of the posterior capsule develops it is essential that the connective tissue function with the joint be addressed in addition to restoring normal mechanics of your arm and shoulder while treating trigger points in the teres minor
If treatment is limited to this individual muscle without addressing the mechanics of the entire joint will fail and pain relief will be temporary.
You can also stretch the teres minor in similarly to infraspinatus but you may feel it differently.
You can deepen this stretch by using reciprocal inhibition to activate the antagonists of the infraspinatus and teres minor.
Following pressure release or stretching a cold pack may be helpful.
If tightness of the posterior capsule develops it is essential that the connective tissue function with the joint be addressed in addition to restoring normal mechanics of your arm and shoulder while treating trigger points in the teres minor
If treatment is limited to this individual muscle without addressing the mechanics of the entire joint will fail and pain relief will be temporary.
 Avoid sustained or repetitive actions that overload the teres minor muscle such lifting heavy objects overhead, backward or out to the side.
Avoid sustained contraction of the teres minor. For example, 20 minutes or more of hairstyling or work overhead can easily activate this muscle. Take short breaks so give the teres minor a chance to recover.
Avoid sustained or repetitive actions that overload the teres minor muscle such lifting heavy objects overhead, backward or out to the side.
Avoid sustained contraction of the teres minor. For example, 20 minutes or more of hairstyling or work overhead can easily activate this muscle. Take short breaks so give the teres minor a chance to recover.
 Restful sleep may be difficult due to pain. Consider sleeping on the uninvolved side. If you sleep on the pain-free side your sleep will be improved if you support the painful arm on a pillow, avoiding the prolonged lengthening of teres minor that can lead to pain.
Restful sleep may be difficult due to pain. Consider sleeping on the uninvolved side. If you sleep on the pain-free side your sleep will be improved if you support the painful arm on a pillow, avoiding the prolonged lengthening of teres minor that can lead to pain.
 You can also use this a variation of this technique to support the painful arm when sleeping on your back or when sitting.
In general, do not sleep on your stomach. Do not lie on either on your back with your arms extended up over your head. This will externally rotate your arms and keep the teres minor in a shortened position for an extended time.
Engage is self-care activities as recommended here.
You can also use this a variation of this technique to support the painful arm when sleeping on your back or when sitting.
In general, do not sleep on your stomach. Do not lie on either on your back with your arms extended up over your head. This will externally rotate your arms and keep the teres minor in a shortened position for an extended time.
Engage is self-care activities as recommended here.
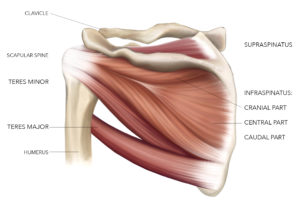
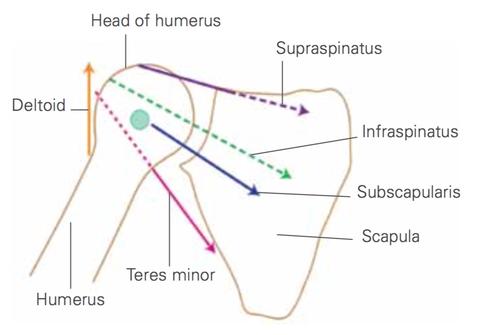
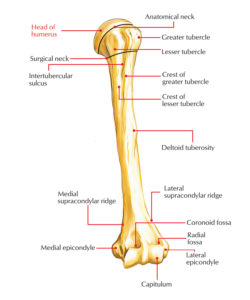
 Teres minor, along with suprapinatus, infraspinatus, and subscapularis insert into the lesser and greater tuberosities on the front and back of your humerus. They form a 'cuff' of connnective tissue and muscles around the head of your humerus that help rotate your arm at the shoulder. Collectively, they are called the rotator cuff.
Teres minor functions much like infraspinatus and is involved in both raising your arm to the side and maintaining stability in your shoulder joint as you do. It also externally rotates your shoulder, as you would when cocking back before a throw.
Teres minor, along with suprapinatus, infraspinatus, and subscapularis insert into the lesser and greater tuberosities on the front and back of your humerus. They form a 'cuff' of connnective tissue and muscles around the head of your humerus that help rotate your arm at the shoulder. Collectively, they are called the rotator cuff.
Teres minor functions much like infraspinatus and is involved in both raising your arm to the side and maintaining stability in your shoulder joint as you do. It also externally rotates your shoulder, as you would when cocking back before a throw.
 Although each of these rotator cuff muscles participate in the rotation of your arm, their primary purpose is to pull the head of humerus fairly tight into the shallow socket of the shoulder blade. Unlike your knee or ankle, this stability is created by largely these rotator cuff muscles, not ligaments. It part of what allows us to have much greater range of motion at our shoulder than any other joint. For this stabilizing function, you could think of them as powered, dynamic ligaments.
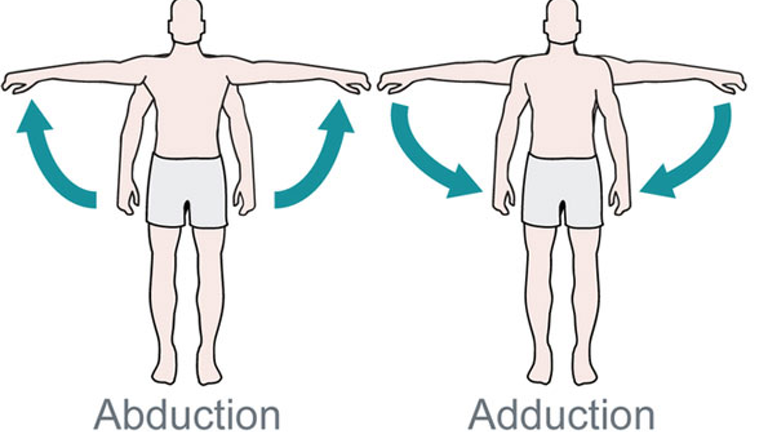
Across various arm positions, teres minor is the strongest external rotator the arm among the rotator cuff muscles. However, teres minor most effective in external rotation with your arm raised to 90 degrees of abduction. External rotation is necessary for full elevation of your arm at the shoulder joint. However, movement at the shoulder joint is a complex, coordinated activity.
Although each of these rotator cuff muscles participate in the rotation of your arm, their primary purpose is to pull the head of humerus fairly tight into the shallow socket of the shoulder blade. Unlike your knee or ankle, this stability is created by largely these rotator cuff muscles, not ligaments. It part of what allows us to have much greater range of motion at our shoulder than any other joint. For this stabilizing function, you could think of them as powered, dynamic ligaments.
Across various arm positions, teres minor is the strongest external rotator the arm among the rotator cuff muscles. However, teres minor most effective in external rotation with your arm raised to 90 degrees of abduction. External rotation is necessary for full elevation of your arm at the shoulder joint. However, movement at the shoulder joint is a complex, coordinated activity.
 Individually, certain rotator muscles are recruited early and different muscles activate later, keeping the head of the humerus stable in most movements.
The structure of the shoulder joint and actions of several muscles coordinate to prevent the head of the humerus from moving down, even under significant load or when you are tired. However, in other positions, we don't have this protection and additional contraction of the rotator cuff muscles, including teres minor, is necessary.
Individually, certain rotator muscles are recruited early and different muscles activate later, keeping the head of the humerus stable in most movements.
The structure of the shoulder joint and actions of several muscles coordinate to prevent the head of the humerus from moving down, even under significant load or when you are tired. However, in other positions, we don't have this protection and additional contraction of the rotator cuff muscles, including teres minor, is necessary.
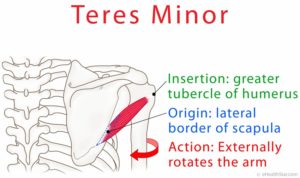
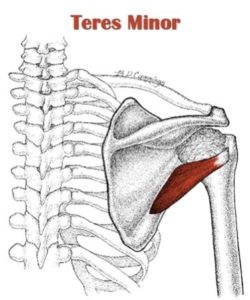 The teres minor (Latin teres meaning 'rounded') is a narrow, elongated muscle of the rotator cuff. The muscle originates from the outside edge and adjacent rear surface of the scapula and inserts at both the greater tubercle of the humerus and the rear surface of the joint capsule.
The primary function of the teres minor is to modulate the action of the deltoid, preventing the humeral head from sliding upward as the arm is abducted. It also externally rotates the arm.
The teres minor (Latin teres meaning 'rounded') is a narrow, elongated muscle of the rotator cuff. The muscle originates from the outside edge and adjacent rear surface of the scapula and inserts at both the greater tubercle of the humerus and the rear surface of the joint capsule.
The primary function of the teres minor is to modulate the action of the deltoid, preventing the humeral head from sliding upward as the arm is abducted. It also externally rotates the arm.
Structure
 Teres minor arises from the back surface of the border of the scapula near the armpit for the upper two-thirds of its extent, and from two fascial sheets. One normally separates it from the infraspinatus muscle, the other from the teres major muscle.
Its fibers run diagonally upwards and out to the shoulder joint. The upper fibers ones end in a tendon that is inserted into the lowest of the three impressions on the greater tubercle of the humerus; the lowest fibers are inserted directly into the humerus immediately below this impression.
Teres minor arises from the back surface of the border of the scapula near the armpit for the upper two-thirds of its extent, and from two fascial sheets. One normally separates it from the infraspinatus muscle, the other from the teres major muscle.
Its fibers run diagonally upwards and out to the shoulder joint. The upper fibers ones end in a tendon that is inserted into the lowest of the three impressions on the greater tubercle of the humerus; the lowest fibers are inserted directly into the humerus immediately below this impression.