 The triceps brachii (three-headed upper arm) muscle is a large muscle of the back of the upper arm. It is the primary muscle used for elbow extension (straightening the arm).
The triceps brachii (three-headed upper arm) muscle is a large muscle of the back of the upper arm. It is the primary muscle used for elbow extension (straightening the arm).
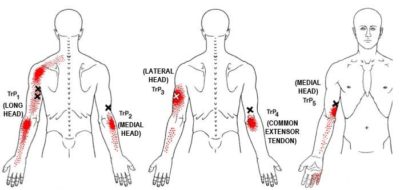
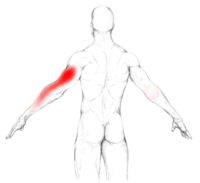
Trigger points occur in all three heads but referred pain from the long head is the most common. Referred pain from the long head occurs up and down the back of the arm and to the lateral (outside) epicondyle (bony bump) with a spill-over pattern between the shoulder and neck. Trigger points in the lateral head refer to the middle, back of the upper arm, and may include the fingers. The medial head refers to the medial (inner) epicondyle, forearm, and fingers. The anconeus referral pattern is small, focused on the lateral epicondyle.
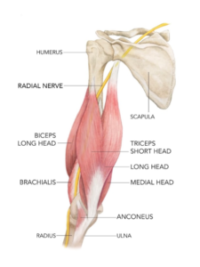
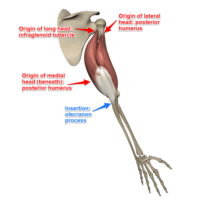
The long head originates on the shoulder blade. The other two heads originate on the humerus (upper arm bone). All three heads converge into a single attachment on the ulna (forearm bone running from the elbow to the little finger side of the wrist).
All three heads extend the elbow but the medial head is the prime mover. The long head also adducts and assists in extending the arm at the shoulder. The anconeus muscle, sometimes called the fourth head, is an extension of the triceps below the elbow that provides stability.
Biceps brachii trigger points are typically activated from repetitive or stress overload in activities that involve straightening your arm. Examples include desk work, driving, or other handwork without effective elbow support.
Corrective actions include trigger point pressure release, stretching, and avoiding or modifying activities that overload the muscle.
If you maintain a posture or activity that activates a trigger point in any muscle it will continue.
 Trigger points can be activated anywhere in the triceps from unaccustomed or repetitive loading, especially in a poorly conditioned muscle.
Trigger points can be activated anywhere in the triceps from unaccustomed or repetitive loading, especially in a poorly conditioned muscle.
TrP1 in the long head is located deep, in the middle, and slightly towards the inside of the back of the arm. This the most common triceps trigger point and refers both up into the shoulder and down to the lateral epicondyle and down the radial (thumb) side of the forearm.
The tiny anconeus muscle is an extension of the triceps below the elbow. Its pain pattern projects near the bony point of the elbow, towards the outside.
 Activities that extend the arm at both the elbow and the shoulder, such as using a manual transmission, can overload the long head. Activities that require adduction (pulling in) of the arm also stress the long head. Think pushups, bench presses, golf, or a backhand mis-hit in tennis.
Activities that extend the arm at both the elbow and the shoulder, such as using a manual transmission, can overload the long head. Activities that require adduction (pulling in) of the arm also stress the long head. Think pushups, bench presses, golf, or a backhand mis-hit in tennis.

Any activity that requires you to use your hands in front of your body without elbow support stress all three heads. This includes desk work without a proper chair, needlepoint, and using tools and fasteners against a vertical surface.
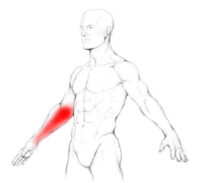
TRP2 and TRP3 are in the medial and lateral heads, respectively. Their pain patterns run down the associated side of the arm, but TRP2 in the medial head refers entirely below the below and TRP3 refers from the middle of the arm to the fingers, skipping the elbow and wrist.
The TRP5 pattern extends from just above the inside of the elbow, down the forearm, and into the fourth and fifth fingers, skipping the wrist.
TRP4 is caused by the combined actions of the other trigger points and cannot be relieved with pressure release.
Placing any muscle in a shortened or lengthened position for an extended period of time can also activate trigger points in the muscle.
Myofascial self-care always starts with establishing a foundation of diaphragmatic breathing. Once you have taken a few moments to get in touch with your breath, we move on to self-compression.
 You can use self-pressure release for the triceps while seated, standing, or in side-lying positions, but you will have more control standing.
You can use self-pressure release for the triceps while seated, standing, or in side-lying positions, but you will have more control standing.
Using your hand from the unaffected side, gather your fingers together to reinforce each other. Extend the affected arm and gently grasp the muscle and run your hand over the length of it. You probably won’t feel the different heads, but it runs the entire length of your upper arm.
Explore the muscle with your hand, note areas that are sorer, and bring your focus to them. Gently extend and contract your elbow and continue searching. Find the tender spot and apply pressure for up to 30 seconds as pain decreases. You can do this three to five times.
There are other techniques using balls or rollers to focus on specific areas, but they can be cumbersome and too aggressive. Blood vessels and nerves in the arm are superficial, so any self-release should be done with caution. If you feel tingling or circulation changes in your hand you should reposition and take a different approach.
In the physical therapy world, triceps trigger points are often treated as “triceps tendonitis” but many of the self-care tips are similar:
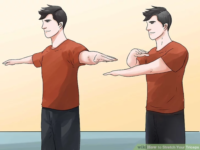
After completing self-compressions, move your arm through its range of motion and prepare to gently stretch your triceps.
You can use your breath to deepen each stretch. Begin with a generous inhale and as you exhale, gently stretch by rotating the body away from the doorframe. You can repeat this sequence three to five times, up to four times per day.



If you experience pain following pressure release and stretching, a cold pack may be helpful.
Because the triceps have three separate sections with multiple trigger points in some, the pain patterns are a little complicated and overlap considerably. Pain in the upper arm and shoulder tends to be vague and hard to locate. Many people are not aware of range of motion limitations (inability to extend the elbows) or compensations for a shortened reach, like additional movement of the shoulder blade or the body. Pain is worst during activities that require forceful extension of the elbow. As the activity of these trigger points increases, they often contribute to a painful diagnosis of “tennis elbow” and a significant loss of function.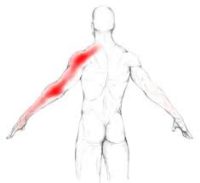
TrP1 in the long head is located deep, in the middle, and slightly towards the inside of the back of the arm. This the most common triceps trigger point and refers both up into the shoulder and down to the lateral epicondyle and down the radial (thumb) side of the forearm. Note that this pattern overlays the combination of the other four referral patterns.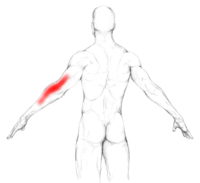
TRP2 lies in the medial head. However, the pain pattern runs down the outside (thumb side) of the forearm from just below the elbow to above the wrist.
 TRP3 is in the lateral head. Its pain pattern runs from the middle of the upper arm to the fingers, skipping the elbow and wrist.
TRP3 is in the lateral head. Its pain pattern runs from the middle of the upper arm to the fingers, skipping the elbow and wrist.
 The TRP5 pattern extends from just above the inside of the elbow, down the forearm, and into the fourth and fifth fingers, skipping the wrist.
The TRP5 pattern extends from just above the inside of the elbow, down the forearm, and into the fourth and fifth fingers, skipping the wrist.
 TRP4 is caused by the combined actions of the other trigger points. It is a connective tissue inflammation, not a traditional trigger point, and cannot be relieved with pressure release.
TRP4 is caused by the combined actions of the other trigger points. It is a connective tissue inflammation, not a traditional trigger point, and cannot be relieved with pressure release.
Avoid repetitive actions that overload the muscle, such as extension of your elbow or using your hands without your elbows supported.
 During desk work, your upper arm should be nearly vertical, with your elbows behind the front of your chest. They should not project forward. Many of us sit too far away from our desks and are not close enough to keep our arms straight.
During desk work, your upper arm should be nearly vertical, with your elbows behind the front of your chest. They should not project forward. Many of us sit too far away from our desks and are not close enough to keep our arms straight.
An armrest should support your elbow at the correct height for the work you are doing.
Some people have relatively short upper arms in relation to their bodies. If you bend your elbows, they should reach the top of the bony crest of your hip. If not, your upper arms are shorter and it will limit your reach. You may benefit from a keyboard tray at your desk. It also makes an adjustable armrest even more important.
 In fitness activities, it may help to reduce loading on the triceps. Pushups can be modified by placing the hands wider to shift load from the triceps to the pecs. Consider staggered pushups to transfer more of the load to your core.
In fitness activities, it may help to reduce loading on the triceps. Pushups can be modified by placing the hands wider to shift load from the triceps to the pecs. Consider staggered pushups to transfer more of the load to your core.
Reduce the weight in bench presses temporarily. Tennis players may benefit from a lighter racket. Golf players should consciously reduce their drive.
Strength training should be done more slowly and meditatively, with a focus on using your breath.
 The triceps crosses both the shoulder and elbow, but the main function is at the elbow where it extends the forearm.
The triceps crosses both the shoulder and elbow, but the main function is at the elbow where it extends the forearm.
The triceps is an extensor muscle of the elbow joint and an antagonist of the biceps and brachialis muscles.  It can also fixate the elbow joint when the forearm and hand are used for fine movements, e.g., when typing or writing.
It can also fixate the elbow joint when the forearm and hand are used for fine movements, e.g., when typing or writing.
The long head assists with sustained force generation, or when synergistic control of the shoulder, elbow, or both are needed. The lateral head is used for movements requiring occasional high-intensity force such as a tennis swing while the medial head engages for more precise, low-force movements.
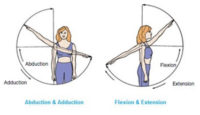 Originating on the scapula, the long head also acts on the shoulder joint and is also involved in extension or extension and adduction of the arm at the shoulder. It also helps stabilize the shoulder joint at the top of the humerus.
Originating on the scapula, the long head also acts on the shoulder joint and is also involved in extension or extension and adduction of the arm at the shoulder. It also helps stabilize the shoulder joint at the top of the humerus.
The triceps brachii is a large muscle on the front of the upper arm between the shoulder and the elbow. 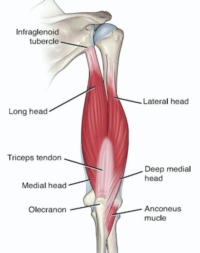 Both heads of the muscle arise on the shoulder blade and join to form a single muscle belly that is attached to the upper forearm.
Both heads of the muscle arise on the shoulder blade and join to form a single muscle belly that is attached to the upper forearm.
Structure
The long head arises from the infraglenoid tubercle of the scapula. “Infra” means under, “glenoid” means shoulder socket and “tubercle” means bony bump; it attaches to a bony bump just under the shoulder socket. It extends down and to the front in between the teres minor and the teres major.
The medial head arises near the top of the humerus, from the back surface; from the medial intermuscular septum; and its lower part also arises from the lateral intermuscular septum. The medial head is mostly covered by the lateral and long heads and is only visible at the lowest part of the humerus.
The lateral head arises from the back surface of the humerus, from the greater tubercle of the arm, down to the region of the lateral intermuscular septum.
Each of the three triceps muscle bodies has its own motorneuron subnucleus in the motor column in the spinal cord. The medial head is formed predominantly by small type I fibers and motor units, the lateral head of large type IIb fibers and motor units, and the long head of a mixture of fiber types and motor units. It has been suggested that each muscle body “may be considered an independent muscle with specific functional roles.”
The fibers converge to a single tendon to insert onto the bony point of the elbow, which is part of the ulna, and to the posterior wall of the capsule of the elbow joint where bursae (cushion sacks) are often found. Some research indicates that there may be more than one tendon. Parts of the common tendon radiate into the fascia of the forearm and can almost cover the anconeus muscle.
 For example, in a biceps curl, you would use a concentric contraction of your biceps, coupled with an eccentric contraction of your triceps, to flex your elbow and push the weight up. As you lower the weight, eccentric contractions of your biceps are required to maintain control and prevent dropping the weight.
For example, in a biceps curl, you would use a concentric contraction of your biceps, coupled with an eccentric contraction of your triceps, to flex your elbow and push the weight up. As you lower the weight, eccentric contractions of your biceps are required to maintain control and prevent dropping the weight.
Isotonic Contractions
Isotonic contractions maintain constant tension in the muscle as the muscle changes length. This can occur only when a muscle’s maximal force of contraction exceeds the total load on the muscle. Isotonic muscle contractions can be either concentric (muscle shortens) or eccentric (muscle lengthens).Concentric Contractions
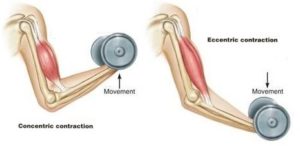
A concentric contraction is a type of muscle contraction in which the muscle shortens while generating force. This is typical of muscles that contract due to the sliding filament mechanism, and it occurs throughout the muscle. Such contractions also alter the angle of the joints to which the muscles are attached.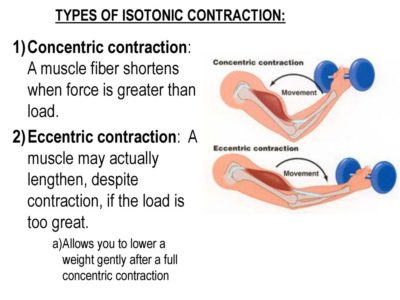 This occurs throughout the length of the muscle, generating force; causing the muscle to shorten and the angle of the joint to change. For instance, a concentric contraction of the biceps would cause the arm to bend at the elbow as the hand moves close to the shoulder (a biceps curl).
A concentric contraction of the triceps would change the angle of the joint in the opposite direction, straightening the arm and moving the hand away from the shoulder.
This occurs throughout the length of the muscle, generating force; causing the muscle to shorten and the angle of the joint to change. For instance, a concentric contraction of the biceps would cause the arm to bend at the elbow as the hand moves close to the shoulder (a biceps curl).
A concentric contraction of the triceps would change the angle of the joint in the opposite direction, straightening the arm and moving the hand away from the shoulder.
Eccentric Contractions
An eccentric contraction results in the lengthening of a muscle. These contractions decelerate muscles and joints (acting as “brakes” to concentric contractions) and can alter the position of the load force. During an eccentric contraction, the muscle lengthens while under tension due to an opposing force that is greater than the force generated by the muscle. However, rather than working to pull a joint in the direction of the muscle contraction, the muscle acts to decelerate the joint at the end of a movement or otherwise control the repositioning of a load. This can occur involuntarily (when attempting to move a weight too heavy for the muscle to lift) or voluntarily (when the muscle is “smoothing out” a movement). Strength training involving both eccentric and concentric contractions appears to increase muscular strength and joint stability more than training with concentric contractions alone.Isometric Contractions
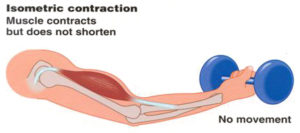 In contrast to isotonic contractions, isometric contractions generate force without changing the length of the muscle. This is typical of muscles found in the hands and forearm: the muscles do not change length, and joints are not moved, so force for grip is sufficient. An example is when the muscles of the hand and forearm grip an object; the joints of the hand do not move, but muscles generate sufficient force to prevent the object from being dropped.
For people with hypermobile joints, strength training can be a challenge. Tension stresses the connective tissues of the joint as force is transmitted through its range of motion. Isometric exercises can be ideal in these circumstances because there is minimal movement. This means that the joint is placed into vulnerable hyperextended positions under force.
In contrast to isotonic contractions, isometric contractions generate force without changing the length of the muscle. This is typical of muscles found in the hands and forearm: the muscles do not change length, and joints are not moved, so force for grip is sufficient. An example is when the muscles of the hand and forearm grip an object; the joints of the hand do not move, but muscles generate sufficient force to prevent the object from being dropped.
For people with hypermobile joints, strength training can be a challenge. Tension stresses the connective tissues of the joint as force is transmitted through its range of motion. Isometric exercises can be ideal in these circumstances because there is minimal movement. This means that the joint is placed into vulnerable hyperextended positions under force. You can develop amazing strength without free weights, machines, or resistance bands.
One of the original bodybuilder gurus from the 1920s, Charles Atlas, based his workouts primarily on isometric exercises, eventually even trademarking a term for his exercise method that he called "Dynamic Tension."
If you have hypermobile joints you can strength train safely at home with isometric exercises.
You can develop amazing strength without free weights, machines, or resistance bands.
One of the original bodybuilder gurus from the 1920s, Charles Atlas, based his workouts primarily on isometric exercises, eventually even trademarking a term for his exercise method that he called "Dynamic Tension."
If you have hypermobile joints you can strength train safely at home with isometric exercises.